
Lymphangioma of the Left Neck in a 56-Year-Old Male
A 56-year-old male presented with a one-year history of a progressively enlarging mass on the left side of the neck. The swelling was painless and not associated with systemic symptoms. His medical history was significant for hypertension, well controlled with medication. He had no prior surgical history, and no known drug allergies were reported.
SURGERYHEAD AND NECKVIDEO
9/9/20252 min read
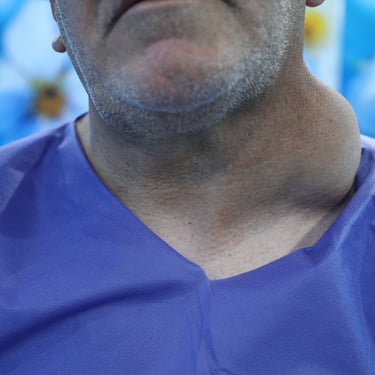
Presentation and History:
A 56-year-old male presented with a one-year history of a progressively enlarging mass on the left side of the neck. The swelling was painless and not associated with systemic symptoms. His medical history was significant for hypertension, well controlled with medication. He had no prior surgical history, and no known drug allergies were reported.
Laboratory Investigations:
Routine laboratory evaluation revealed the patient was euthyroid, with a normal complete blood count and inflammatory markers (CRP and ESR).
Initial Imaging Studies:
Ultrasound of the Neck demonstrated a large, well-defined cystic lesion in the left side of the neck, measuring approximately 12.3 × 10.9 × 7.9 cm. The lesion extended into the supraclavicular region, posterior triangle, and lower neck. It showed a thin wall (~2 mm), internal fine echoes, and thin septations without solid components. The mass exerted a compressive effect on the trachea, thyroid, and left common carotid artery, displacing them anterolaterally to the right side. There were no features suggestive of invasion. The thyroid gland appeared normal in size and echotexture with preserved vascularity, and no abnormal cervical lymphadenopathy was identified. The submandibular and parotid glands were normal. The impression favored a lymphangioma.
MRI of the Neck with Contrast further characterized the lesion as a 12 × 10 × 7.5 cm thin-walled cyst extending from the anterior and posterior triangles of the left neck, with a component extending posterior to the left clavicle and retrosternally down to the origin of the left subclavian artery. The lesion was located deep to the sternocleidomastoid muscle, demonstrated multiple thin septations, and showed no evidence of hemorrhage or infection. There was significant mass effect on the adjacent left internal jugular vein, which was not visualized—raising suspicion of compression versus chronic thrombosis. Partial encasement of the left common and internal carotid arteries was noted. The thyroid, salivary glands, pharynx, larynx, and cervical lymph nodes were unremarkable.
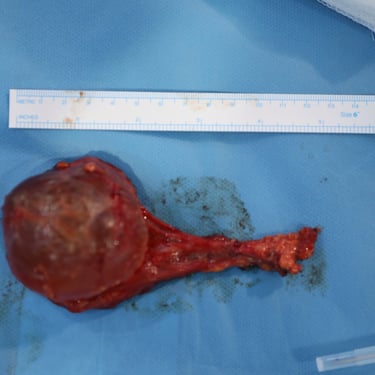
Surgical Management:
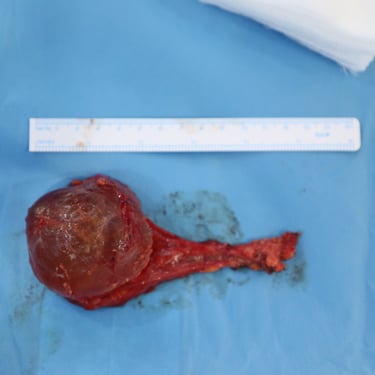
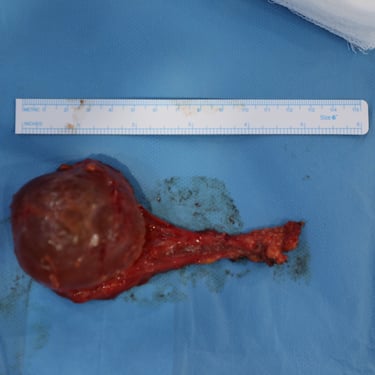
The patient underwent surgical excision of the left-sided neck mass under general anesthesia, along with excision of a concurrent left scalp lesion for cosmetic reasons. The excised specimens included:
Left neck mass.
Left scalp lesion (oriented with superior short and posterior long sutures).
No preoperative fine needle aspiration or prior histopathological evaluation had been performed.
Histopathology Report:
Left Neck Cyst: Lymphangioma with benign lymph nodes; no evidence of malignancy.
Scalp Lesion: Seborrheic keratosis with sebaceous gland hyperplasia; no evidence of malignancy.




Address
Majid Bag Main Street, Beside University of Sulaymaniyah Old Campus, Madam Mitterrand, Sulaymaniyah, Iraq
Contacts
info@ssthyroid.com

