
Recurrent Multifocal Pleomorphic Adenoma of the Right Parotid Gland in a 37-Year-Old Male
A 37-year-old male presented with a long-standing right infra-auricular swelling that had been gradually increasing in size over a three-year period. The swelling was painless and unassociated with facial weakness, trismus, or constitutional symptoms. His past medical history was unremarkable; however, he had undergone surgery in the same anatomical region approximately 15 years earlier, raising suspicion for recurrence of a parotid gland neoplasm, particularly given the slow and progressive clinical course.
SURGERYHEAD AND NECKVIDEO
12/2/20252 min read


Patient Presentation:
A 37-year-old male presented with a long-standing right infra-auricular swelling that had been gradually increasing in size over a three-year period. The swelling was painless and unassociated with facial weakness, trismus, or constitutional symptoms. His past medical history was unremarkable; however, he had undergone surgery in the same anatomical region approximately 15 years earlier, raising suspicion for recurrence of a parotid gland neoplasm, particularly given the slow and progressive clinical course.
Ultrasound Findings:
Ultrasound examination of the neck revealed a normal-sized right parotid gland with preserved parenchymal echogenicity. Multiple adjacent solid, hypoechoic, mildly vascular nodules of varying sizes were identified in both the superficial and deep lobes of the mid–upper third of the gland. The largest measured 21 × 17 × 11 mm. Several nodules extended to subcutaneous tissues on the surface of the gland, with one small nodule (~3 mm) situated near the upper pole, partially outside the gland. These features, combined with the patient’s prior surgical history, strongly suggested recurrent pleomorphic adenoma. Both lobes of the thyroid gland were normal with homogeneous echotexture, showing only a tiny 2 mm TR1 nodule in the left lobe. No significant cervical lymphadenopathy was present, and the submandibular and left parotid glands appeared normal.
MRI Findings:
MRI of the neck with intravenous gadolinium contrast demonstrated a multiloculated lesion measuring 5.2 × 2.4 × 1.8 cm involving the superficial lobe of the right parotid gland, extending toward the preauricular region. The lesion exhibited peripheral enhancement with internal cystic components—an imaging profile characteristic of pleomorphic adenoma, including its recurrent presentations. The radiologist recommended tissue diagnosis for confirmation, as recurrent pleomorphic adenomas may present with multifocal or multinodular patterns, especially following prior surgery.
Cytology (FNA):
Fine-needle aspiration cytology was performed and classified as Benign (Category IVA) according to the Milan System for Reporting Salivary Gland Cytopathology. The cytologic appearance was suggestive of pleomorphic adenoma, showing a mixture of epithelial and stromal elements consistent with a benign mixed salivary gland tumor. Although FNA is highly supportive in diagnosis, the multifocal nature of the nodules and prior operative history underscored the need for surgical excision due to the risk of progressive recurrence.
Surgical Management:
Given the clinical, radiologic, and cytologic findings consistent with recurrent pleomorphic adenoma, the patient underwent a right total parotidectomy. The surgical approach aimed to remove all multifocal nodules while preserving the facial nerve. Due to scarring and anatomical alteration from the prior surgery, meticulous dissection was required, but the procedure proceeded without intraoperative complications.
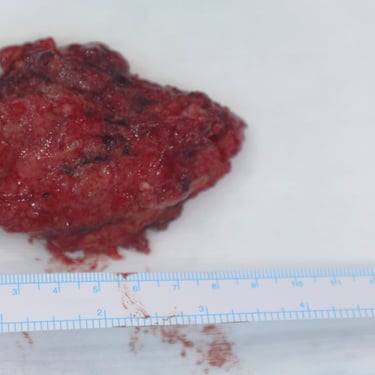
Histopathological Examination:
Histopathology of the surgical specimen confirmed the presence of multiple pleomorphic adenomas (benign mixed tumors) within the right parotid gland. No malignant transformation was identified. The multifocal pattern was consistent with recurrent disease, a known behavior of pleomorphic adenoma following prior incomplete excision or capsular breach.
Postoperative Course and Follow-Up:
The patient’s postoperative recovery was smooth, with no significant complications. He exhibited no evidence of facial nerve weakness or neuropraxia during hospitalization or follow-up visits. The surgical site healed well, and there were no early signs of recurrence. Continued long-term surveillance was recommended due to the known potential for late recurrences in pleomorphic adenoma, especially in previously operated glands.




Address
Majid Bag Main Street, Beside University of Sulaymaniyah Old Campus, Madam Mitterrand, Sulaymaniyah, Iraq
Contacts
info@ssthyroid.com

