
Recurrent Suspicion Following Low-Grade Mucoepidermoid Carcinoma of the Left Parotid in a 22-Year-Old Female
A 22-year-old female presented with a left preauricular swelling, which had been gradually increasing in size. She reported no associated symptoms such as facial weakness, pain, or systemic complaints. Her past medical and surgical history was unremarkable, and she had no history of radiation exposure or familial malignancy.
SURGERYHEAD AND NECK
5/6/20252 min read


Patient Presentation:
A 22-year-old female presented with a left preauricular swelling, which had been gradually increasing in size. She reported no associated symptoms such as facial weakness, pain, or systemic complaints. Her past medical and surgical history was unremarkable, and she had no history of radiation exposure or familial malignancy.
Initial Imaging and Surgical Management:
Neck ultrasound revealed a mildly enlarged left parotid gland with a well-defined, lobulated, predominantly cystic mass measuring 51 × 33 × 27 mm, with a thin internal septation and wall thickness of less than 2 mm. The lesion was consistent with an intra-parotid cyst. Based on these findings, the patient underwent a left superficial parotidectomy.
Histopathology Report – Initial Surgery:
Histopathological examination of the excised mass confirmed the diagnosis of low-grade cystic mucoepidermoid carcinoma of the parotid gland, with a maximum tumor dimension of 4.8 cm, corresponding to T3 disease. The diagnosis warranted close surveillance due to the risk of local recurrence.
Postoperative Course and Follow-Up Imaging:
Seven months after the initial surgery, the patient underwent a follow-up neck ultrasound due to the emergence of new swelling near the previous surgical site. Imaging showed marked skin and subcutaneous tissue thickening along the left parotid bed and a heterogeneous, irregular lesion measuring 29 × 16 × 7 mm, located just posterior to the angle of the mandible. The lesion appeared mildly vascular and was deemed suspicious for recurrence, correlating with a previous suspicious FNA result. Additionally, small bilateral cervical lymph nodes were seen, predominantly on the left side in levels I and II, with the largest node measuring 16 × 5 mm in the left submandibular region.
Oncology Evaluation and Management Plan:
The patient had already received radiotherapy (RT) following her initial surgery. Upon recurrence suspicion, she was referred back to oncology. Given the presence of a new growing lesion in a previously irradiated field, the oncology team determined that re-irradiation was not appropriate. Instead, they recommended surgical re-excision of the lesion along with adequate cervical lymph node dissection, due to the aggressive nature of the disease and prior radiation history.
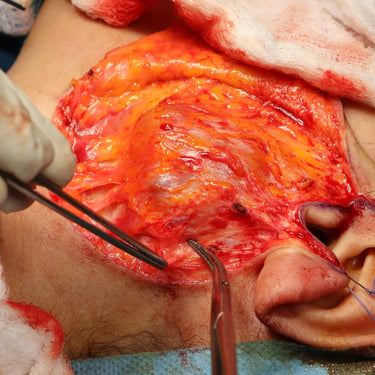
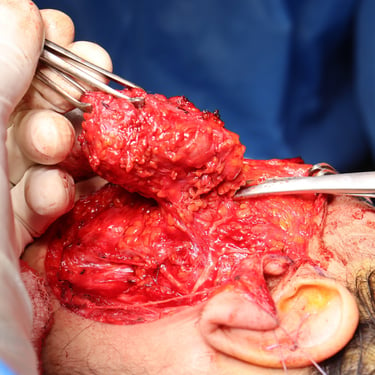
Second Surgical Intervention:
A total parotidectomy was performed to address the suspicious recurrence. The surgery included wide excision of the left parotid bed with the intention of achieving oncologic clearance and staging of potential lymph node involvement.
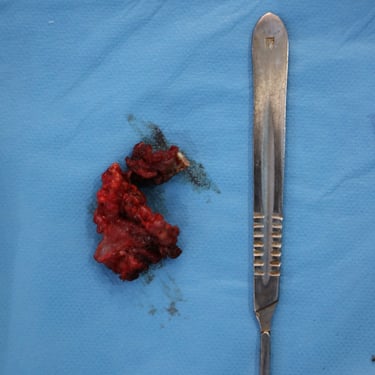
Histopathology Report – Second Surgery:
Histological analysis of the re-excised tissue revealed benign salivary gland tissue, associated with fibrous tissue and skeletal muscle fragments. Diffuse reactive atypia was noted within the salivary tissue, but no residual tumor was identified. These findings suggested a post-treatment reactive process, rather than true tumor recurrence.
Postoperative Follow-Up Imaging:
One week after the second surgery, a follow-up neck ultrasound was performed. The scan showed marked inhomogeneity in the left parotid surgical bed, with a complex hypoechoic, mildly vascular lesion measuring 33 × 28 × 11 mm. This was interpreted as postoperative change or fluid collection, and follow-up imaging was advised to monitor resolution and rule out any late recurrence or complications.
Gallery




Address
Majid Bag Main Street, Beside University of Sulaymaniyah Old Campus, Madam Mitterrand, Sulaymaniyah, Iraq
Contacts
info@ssthyroid.com

