
Right Lower Eyelid Basal Cell Carcinoma Treated with Wide Local Excision and Nasolabial Transposition Flap
A 41-year-old female presented with a lesion on the lateral aspect of her right lower eyelid, which had been progressively enlarging over the past six months. She denied any associated symptoms such as pain, discharge, bleeding, or changes in vision. Her past medical and surgical history was unremarkable, and there were no notable comorbidities or prior dermatological conditions. On physical examination, a small lesion was observed over the lateral right lower eyelid, without surrounding inflammation or ulceration. There was no regional lymphadenopathy, and the rest of the ophthalmologic and systemic examination was within normal limits.
SURGERYHEAD AND NECK
7/22/20252 min read


Clinical Presentation:
A 41-year-old female presented with a lesion on the lateral aspect of her right lower eyelid, which had been progressively enlarging over the past six months. She denied any associated symptoms such as pain, discharge, bleeding, or changes in vision. Her past medical and surgical history was unremarkable, and there were no notable comorbidities or prior dermatological conditions. On physical examination, a small lesion was observed over the lateral right lower eyelid, without surrounding inflammation or ulceration. There was no regional lymphadenopathy, and the rest of the ophthalmologic and systemic examination was within normal limits.
Laboratory and Imaging Investigations:
Ultrasonography of the eyelid revealed a small, ill-defined, heterogeneously hypoechoic lesion measuring approximately 11 mm in length and 1.7 mm in depth. The lesion showed mild peripheral vascularity and was confined to the lateral aspect of the right lower eyelid. The radiologic appearance was suggestive of a basal cell carcinoma. No significant cervical lymphadenopathy was observed on imaging. Laboratory investigations were largely unremarkable: complete blood count (CBC) was within normal limits; serum blood urea was 30.3 mg/dL, serum creatinine was 0.610 mg/dL, and fasting blood glucose was 120 mg/dL.
Surgical Management:
Based on the clinical and radiological suspicion of malignancy, the patient was scheduled for surgical excision. Under general anesthesia and in the supine position, a wide local excision (WLE) of the lesion was performed. Due to the lesion's periocular location and the need for optimal cosmetic and functional outcome, a transposition flap using adjacent nasolabial tissue was designed and mobilized to reconstruct the defect. Hemostasis was achieved meticulously, and the surgical site was closed in layers. The procedure lasted approximately one and a half hours, and the excised tissue was sent for histopathological examination.
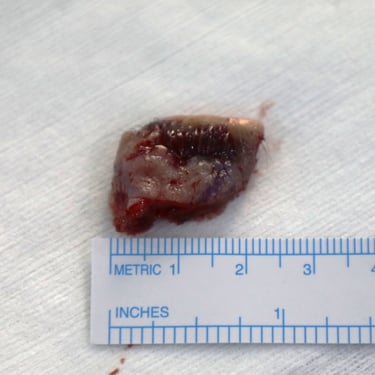
Histopathology Results:
Histological analysis confirmed a diagnosis of nodular basal cell carcinoma. The tumor measured 1.5 cm in greatest dimension and had a thickness of 0.2 cm. It extended into the level of the skeletal muscle bundles of the eyelid. Ulceration was noted on the surface of the tumor, but there was no evidence of lymphovascular or perineural invasion. Importantly, all surgical margins were clear of tumor, though the deep margin was close (<0.1 cm). The inferior and superior outer canthus margins measured 0.3 cm, the medial margin was 0.5 cm, and the lateral margin was 0.7 cm. No additional pathological abnormalities were identified in the examined specimen.
Postoperative Plan:
Given the complete excision with negative margins and the absence of high-risk histological features such as lymphovascular or perineural invasion, no further surgical intervention was deemed necessary. The patient was advised to follow up regularly with both dermatology and ophthalmology for surveillance, focusing on early detection of local recurrence or new lesions. Emphasis was placed on sun protection measures and routine skin checks, particularly given the periocular location and potential cosmetic and functional implications of recurrence.
Gallery





Address
Majid Bag Main Street, Beside University of Sulaymaniyah Old Campus, Madam Mitterrand, Sulaymaniyah, Iraq
Contacts
info@ssthyroid.com

